For those of you who don't believe me when I talk about the problems related to market dominance in health care, I refer you to a recent post by John McDonough, one of the stalwarts of public concern for the health care system. Focusing on Massachusetts, John links us to recent reports produced by the Blue Cross Blue Shield Foundation. John properly expresses "kudos to Massachusetts Health Quality Partners which did the legwork on this terrific resource." He notes:
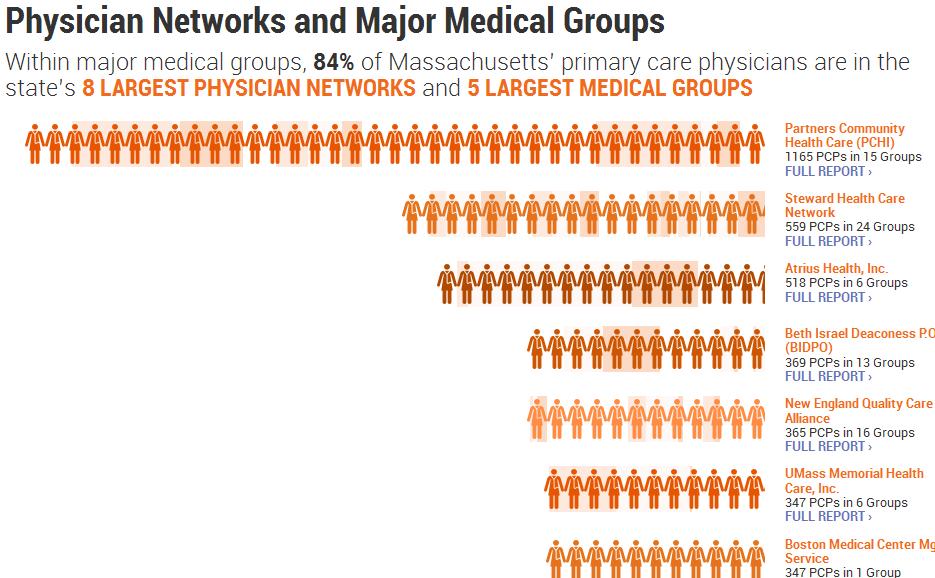
If you want to begin to understand why Partners Healthcare is so dominant in the state's healthcare market, don't go to this page, Hospital Systems by Size, on which Partners is #2 after Steward Health Care System. Go this this page: Physician Networks and Major Medical Groups, where the size of Partners' physician network (called Partners Community Healthcare Inc., PCHI, or "peachy") is larger than #2 (Steward) or #3 (Atrius), combined.


I don't see it listed, but I am guessing that a chart of specialists would be even more skewed to Partners. Remember this chart produced by the system for its presentation to Wall Street?

That helps explain this point raised by John:
Or look at hospitals by Net Patient Service Revenue, and see that Partners total NPSR in 2010 ($4.2 billion) was the same as #s 2 (UMass Memorial), 3 (Steward), and 4 (Beth Israel Deaconess) combined.
John ends his article by saying:
So much more to explore in this highly useful and accessible tool as the state debate over cost and market dominance continues.
Except for one thing: I'm not sure what John means about state debate over market dominance in Massachusetts. Sure, the new state law has a provision that:
Establishes a new “Cost and Market Impact Review” to examine provider organizations to determine whether any provider's market concentration exceeds certain federally-established parameters. If the Commission determines, based on its review, that actions of a provider constitute unfair practices or unfair methods of competition or other violations of law, the Commission must refer the matter to the Attorney General for further action.
The problem is that that game is over. There is no way the Massachusetts AG will have the authority to break up an existing health care system. If s/he tried, the legal process for getting there would take forever.
No, the focus in Massachusetts remains with a misplaced belief that moving the system to one based on capitation will solve the cost problems. (Look at these comments by the chairperson of the state health policy commission.) In addition, there is to be a consideration of the potential for consumer-driven health plans (those with a high deductible component or a health savings account) to influence customer behavior in the selection of doctors and hospitals.
While I am not sanguine about the efficacy of the latter, a condition for its success would be real-time total price and quality transparency, at the consumer level. As Barry Carol notes in a recent comment on this blog, "Perhaps CHIA in MA can lead the way toward true price and quality transparency in healthcare so both patients and referring doctors can much more easily identify the most cost-effective high quality providers and steer their business to them."
If you want to begin to understand why Partners Healthcare is so dominant in the state's healthcare market, don't go to this page, Hospital Systems by Size, on which Partners is #2 after Steward Health Care System. Go this this page: Physician Networks and Major Medical Groups, where the size of Partners' physician network (called Partners Community Healthcare Inc., PCHI, or "peachy") is larger than #2 (Steward) or #3 (Atrius), combined.

I don't see it listed, but I am guessing that a chart of specialists would be even more skewed to Partners. Remember this chart produced by the system for its presentation to Wall Street?
That helps explain this point raised by John:
Or look at hospitals by Net Patient Service Revenue, and see that Partners total NPSR in 2010 ($4.2 billion) was the same as #s 2 (UMass Memorial), 3 (Steward), and 4 (Beth Israel Deaconess) combined.
John ends his article by saying:
So much more to explore in this highly useful and accessible tool as the state debate over cost and market dominance continues.
Except for one thing: I'm not sure what John means about state debate over market dominance in Massachusetts. Sure, the new state law has a provision that:
Establishes a new “Cost and Market Impact Review” to examine provider organizations to determine whether any provider's market concentration exceeds certain federally-established parameters. If the Commission determines, based on its review, that actions of a provider constitute unfair practices or unfair methods of competition or other violations of law, the Commission must refer the matter to the Attorney General for further action.
The problem is that that game is over. There is no way the Massachusetts AG will have the authority to break up an existing health care system. If s/he tried, the legal process for getting there would take forever.
No, the focus in Massachusetts remains with a misplaced belief that moving the system to one based on capitation will solve the cost problems. (Look at these comments by the chairperson of the state health policy commission.) In addition, there is to be a consideration of the potential for consumer-driven health plans (those with a high deductible component or a health savings account) to influence customer behavior in the selection of doctors and hospitals.
While I am not sanguine about the efficacy of the latter, a condition for its success would be real-time total price and quality transparency, at the consumer level. As Barry Carol notes in a recent comment on this blog, "Perhaps CHIA in MA can lead the way toward true price and quality transparency in healthcare so both patients and referring doctors can much more easily identify the most cost-effective high quality providers and steer their business to them."





















